Infectious complications on low and high dose novel induction regimens after pediatric kidney transplantation
Jayanthi Chandar1,3, Marissa Defreitas1,3, Vaka Sigurjonsdottir1,3, Chryso Katsoufis1, Wacharee Seeherunvong1, Carolyn Abitbol1, Mahmoud Morsi2,3, Gaetano Ciancio2,3.
1Pediatric Nephrology, University of Miami , Miami, FL, United States; 2Department of Surgery, University of Miami , Miami, FL, United States; 3Pediatrics and Surgery, Miami Transplant Institute, Miami, FL, United States
Pediatric kidney transplant recipients are vulnerable to clinically significant viral replication (VR) because of their need for intense induction and ongoing need for maintenance immune suppression (ISP).
Objective: In this single-center study we compare the incidence of VR with CMV, EBV, parvovirus, BKV and infectious complications on an induction regimen with rATG consisting of ≥3 mg/kg (hiATG) versus <3mg/kg dose of rATG ( loATG) in the first six months after transplantation. Those who did not receive rATG or received <1mg/kg of rATG constituted noATG.
Methods: Retrospective analysis was performed in 108 patients with an isolated kidney transplant from January 2017 to December 2023. The protocol for hiATG was a cumulative dose of 3mg/kg in the years 2017 -2019 which changed to 1 mg/kg in 2020-2023 for loATG. Those with low pre-transplant vaccine response, low CD4 counts or allergic reaction to rATG received noATG. Induction ISP included 2 doses of basiliximab and methylprednisolone in all patients. VR was defined if PCR was > 137 copies/ml. Discontinuation of anti-metabolites for high-titer viral replication or specific treatment for viral infection defined viral disease. Rejection in the first 6 months was confirmed by kidney biopsy.
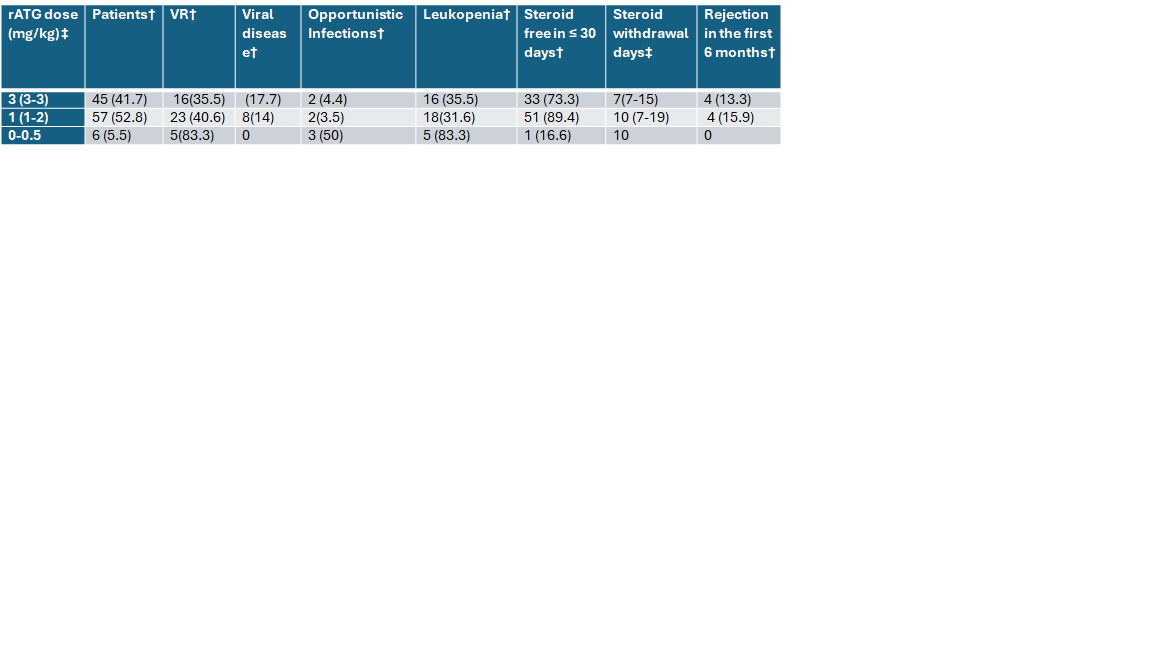
Results: Median age was 13 years (IQR: 7.9-16.0). As seen in Table 1, there were no significant differences in the incidence of VR and rejection between hiATG and loATG in the first 6 months after transplant. Most patients in noATG had VR (See Table 1). Opportunistic infections were observed more often in noATG. Steroid avoidance was possible in both loATG and hiATG. Prevalence of leukopenia was highest in noATG but was seen in both loATG and hiATG. There was no statistically significant difference in rate of rejection between hiATG and loATG.
Conclusions: Infectious complications occur in all induction regimens. In addition, maintenance ISP contributes to lowering host immunity. Differences in host response are likely to play a significant role in propensity to infections, highlighting the importance of individualizing ISP.