
Continuous long term exposure to lower blood pressure stabilizes kidney graft function and improves graft survival in children
Carl Grabitz1, Rizky I. Sugianto1, Ali Duzova2, Kai Krupka3, Burkhard Tönshoff3, Bernhard M.W. Schmidt4, Elke Wühl3, Anette Melk1.
1Department of Pediatric Kidney, Liver, Metabolic and Neurological Diseases, Hanover Medical School, Hannover, Germany; 2Division of Pediatric Nephrology, Faculty of Medicine, Hacettepe University, Ankara, Turkey; 3Center for Pediatrics and Adolescent Medicine, Heidelberg University, Medical Faculty Heidelberg, Heidelberg, Germany; 4Department of Nephrology and Hypertension, Hanover Medical School, Hannover, Germany
CERTAIN Registry.
Introduction: Arterial hypertension has been shown to impact outcome after kidney transplantation in adults. In the pediatric population, arterial hypertension is also highly prevalent. We assessed the effect of blood pressure exposure both on graft function and graft survival in children.
Methods: We analyzed 1,827 patients (1,096 males) from the CERTAIN (Cooperative European Pediatric Renal Transplant Initiative) registry, who received their organ ≤18 years of age and had at least 2 data entries ≥9 months post transplantation. Blood pressure and laboratory measurements were available every 6 months. The cumulative exposure of systolic/diastolic blood pressure percentiles (cSBP/cDBP) was calculated for each visit as the time-averaged area under the curve. CSBP and cDBP was categorized into “≤60th pct”, “61st-90th pct”, and “>90th pct”. Linear and logistic mixed regression models were performed for eGFR and the composite endpoint of graft survival (50% eGFR loss or eGFR≤7 mL/min/1.73m2 or return to dialysis/re-transplant), with cSBP and cDBP as the exposures. The models were adjusted for time since baseline, age at transplantation, sex, donor sex and age, eGFR at baseline, underling disease, and rejection.
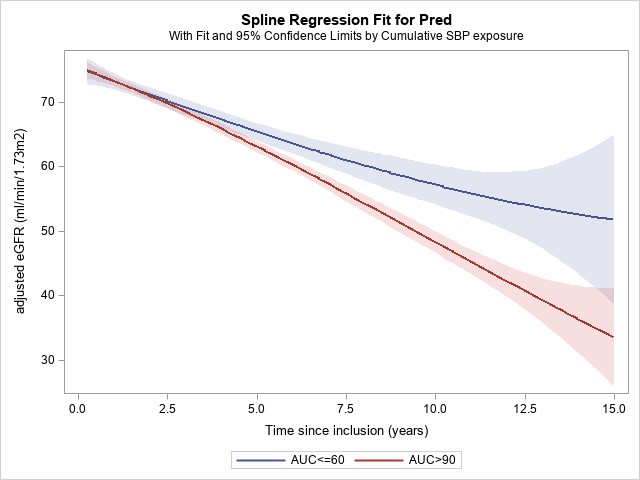
Results: Mean age at transplantation and eGFR at baseline were 9.4±4.9 years and 76.6±26.5 mL/min/1.73m2. Two thirds (68%) of the patients had received a deceased donor kidney and mean follow-up time was 4.0±3.3 years. Blood pressure exposure had a significant impact on graft function. Compared to patients with cSBP of >90th pct, those with cSBP ≤60th pct showed a significantly better graft function (see Figure 1). Compared to patients with cSBP of >90th, those between 61st and 90th pct had a 33% (OR: 0.67, 95% CI 0.47 to 0.97) and those ≤60th pct had a 66% (OR: 0.34, 95% CI 0.19 to 0.61) higher probability of graft survival.
Conclusion: Exposure to low normal blood pressure is associated with better graft function and survival. This calls for an interventional trial to assess intensified blood pressure control after pediatric kidney transplantation.
[1] Arterial Hypertension
[2] Graft Survival
[3] Kidney Transplantation
[4] eGFR
[5] Long Term Outcome