Marco Cugliari, Italy has been granted the CareDx Congress Scientific Awards

BK polyomavirus infection in pediatric renal transplant recipients - A 10 year single center experience
Marco Cugliari1, Sara Testa2, Maria Teresa Ludovica Viganoni1, Silvia Consolo2, Fabio Paglialonga2, Giovanni Montini1,2.
1Department of Clinical Science and Community Health, University of Milan, Milan, Italy; 2Pediatric Nephrology- Dialysis and Transplantation Unit, Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico, Milan, Italy
Aims/Purpose: BK polyomavirus (BKV) is a widespread DNA virus that causes an asymptomatic primary infection in the general population. It then remains quiescent in the cells of the urinary tract. With the use of immunosuppression (IS) in kidney transplant (KTx) recipients, its reactivation or primary infection can cause nephropathy and possibly graft loss. The aim of this study was to describe the incidence of BKV infection, with associated risk factors and outcomes, in pediatric KTx recipients.
Methods: We retrospectively analyzed the data of all KTx recipients from our Pediatric Nephrology center in Milan from January 2014 to February 2024. We only included patients (pts) with a minimum follow-up of 1 yr after Tx, who underwent regular monitoring of BKV viremia. Exclusion criteria were immediate graft failure and age at Tx >21 yrs.
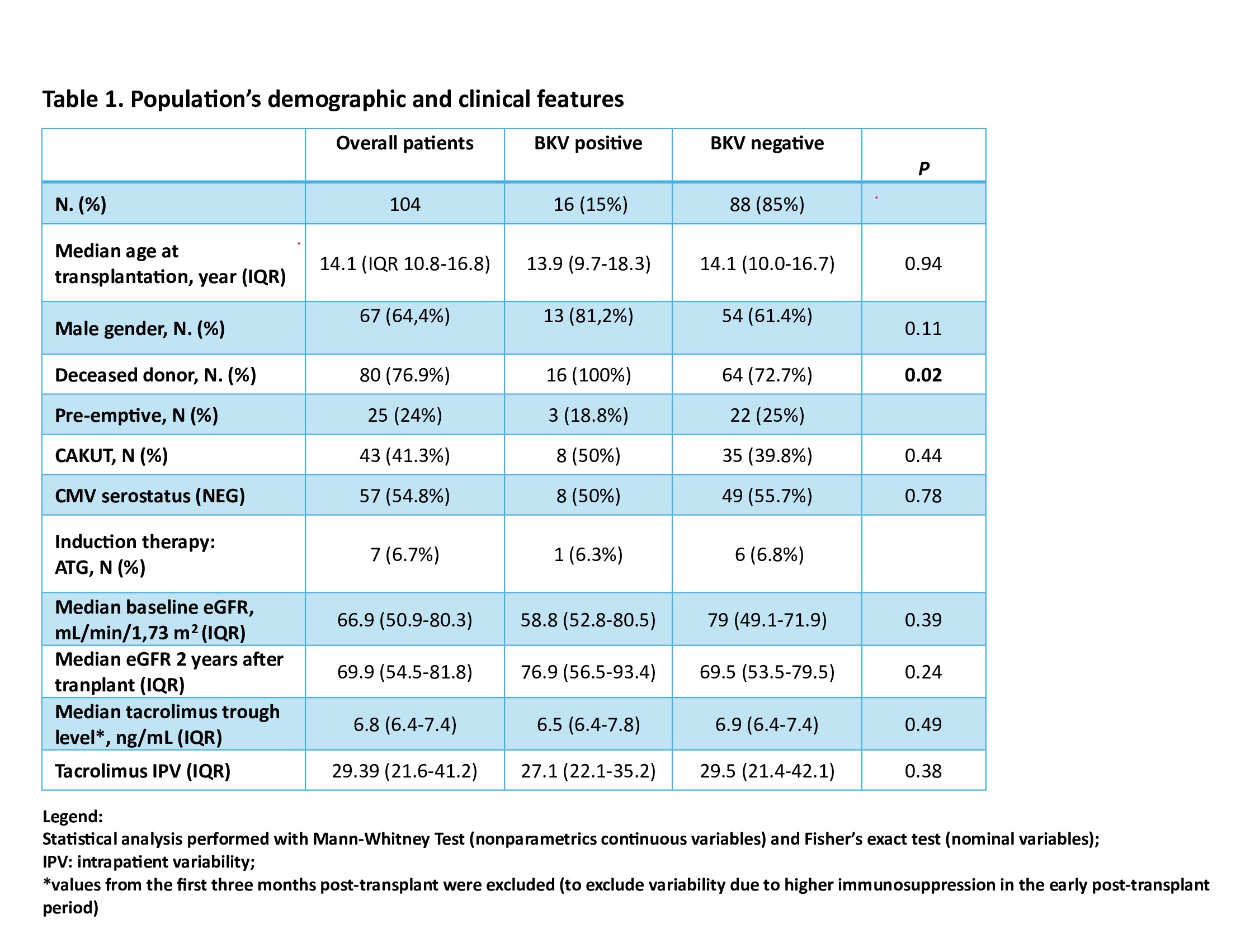
Results: A total of 104 pts were included in the study. The median age at Tx was 14,1 yrs (10.8-16.8). Over the follow-up period, 15.4% (16/104) of pts developed BKV infection. The clinical characteristics of the cohort are shown in table 1. The median time to first BKV detection was 199 days after Tx (IQR: 95-297.5); median BKV DNA peak was 31390 copies/ml (IQR: 3819-78631); median duration of infection was 118 days (IQR: 56-394). Out of the variables analyzed, only the type of kidney donor (deceased) was associated with a higher risk of BKV infection. Within BKV positive pts, 68.8% (11/16) received reduction of IS. All pts but one (who has a recent ongoing infection) became negative. Resolution of BKV infection occurred after a median of 118 days (56-394); pts with IS reduction experienced a shorter median duration of infection (66 vs 119 days, respectively). None of the infected pts presented any sign of nephropathy (eGFR decline and/or proteinura), hence no allograft biopsy was performed. The reduction of IS in pts with BKV infection was not associated with an increase in rejection episodes.
Conclusion: Our data confirms that BKV infection affects a significant proportion of pediatric KTx recipients, underlying the importance of monitoring BKV viremia regularly. Contrary to other reports in the literature, none of our pts showed signs of BKV nephropathy. A possible reason for this difference is that in most other series, pts were younger at Tx than in our cohort. It is thought that young children, who have not been previously exposed to the virus, may be more likely to acquire a primary and more severe infection.
[1] BK polyomavirus
[2] renal transplant