Chief of Transplantation
Division of Transplant Services
SUNY Upstate Medical University
Effects of the kidney allocation system changes in 2014, on the outcomes of kidney transplants in pediatric patients: a retrospective analysis
Mahmoudreza Moein1, Mehrdad Savabi Far2, Reza Saidi1.
1Department of Surgery/ Division of Transplant Services, SUNY Upstate Medical University, Syracuse, NY, United States; 2Dipartimento Medico-Chirurgico di Internistica Clinica e Sperimentale, University of Campania "Luigi Vanvitelli", Naples, Italy
Background: Kidney transplantation (KT) is the preferred treatment for pediatric end-stage renal disease (ESRD) patients, offering better outcomes and quality of life compared to dialysis. In December 2014, a revised Kidney Allocation System (KAS) was implemented to address several shortcomings of the previous allocation process. The primary objectives were to improve post-transplant survival, optimize kidney utilization, and enhance access for disadvantaged candidates. This study aims to evaluate the justification for these changes and assess the impact of the new allocation system.
Material and Method: A retrospective cohort analysis of the SRTR database was done for kidney transplants that were performed for patients younger than 18 years old in the United States from January 2000 to May 2023.
Results: After applying the inclusion and exclusion criteria, a total of 17,498 kidney transplant (KT) cases were included in the final analysis. The study cohort was divided into two groups based on the implementation date of the new allocation system: 11,426 KTs performed from 2000 to 2014, and 6,072 KTs conducted from 2015 to May 2023.
Apart from the mean Kidney Donor Profile Index (KDPI), which was slightly higher in the 2000-2014 group (18% vs. 12%, P < 0.001), other donor and recipient demographics were clinically similar between the two groups.
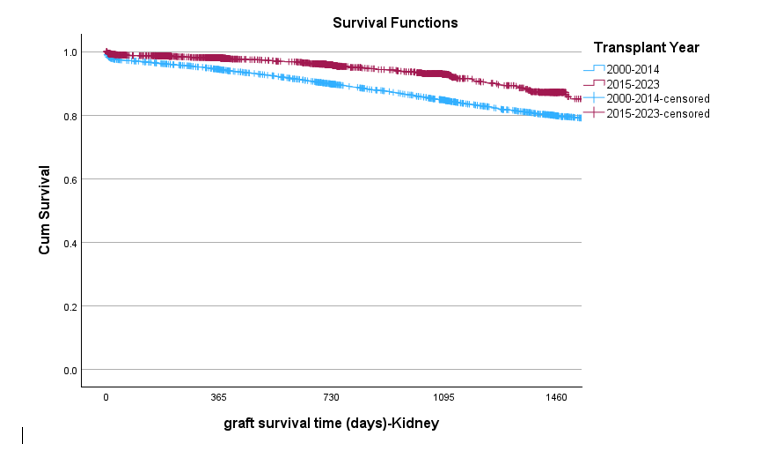
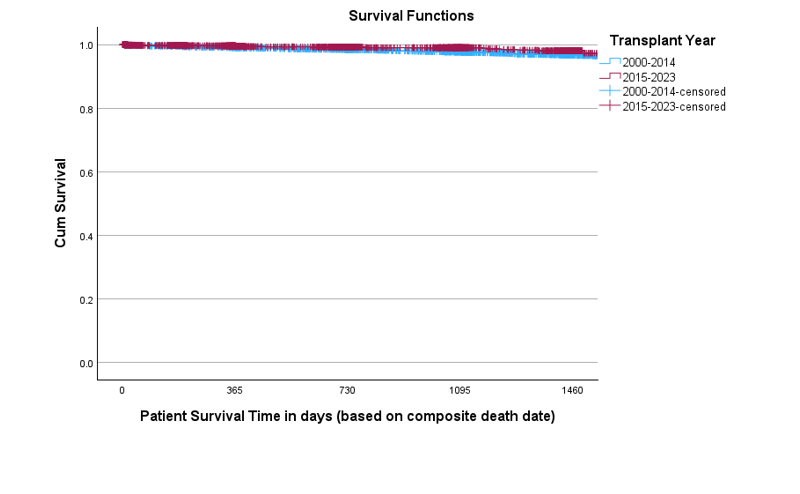
Data analysis revealed a significantly higher 4-year allograft survival rate in the 2015-2023 group compared to the 2000-2014 group (85% vs. 79%, P < 0.01). However, the 4-year patient survival rates were comparable between the two groups.
Chronic rejection, acute rejection, and graft thrombosis were the most common causes of graft failure in both groups. Chronic rejection was significantly more prevalent in the 2000-2014 group (40.6% vs. 28.1%; OR: 1.74, 95% CI: 1.17-2.59). Conversely, graft thrombosis was more frequent in the 2015-2023 group (11.7% vs. 3.9%; OR: 3.25, 95% CI: 1.81-5.94). There was no statistically significant difference in the incidence of acute rejection between the two groups (25% vs. 21%, P = 0.29).
Conclusions: We conclude that the modification of the kidney allocation system for pediatric transplants was successful in improving outcomes and may also contribute to a more equitable distribution of available allografts.
References:
[1] Kidney Transplantation
[2] Pediatric
[3] Kidney allocation system
[4] Policy
[5] SRTR
[6] allograft survival
[7] Outcomes