Living donor plus domino liver transplantation for MSUD: Expanding donor pool safely
Eduardo Antunes da Fonseca1, Carolina Magalhães Costa1, Nathália P. R. Travassos1, Hsiang Wei Teng1, Marcel R. Benavides1, Karina Roda1, Irene Kazuo Miura1, Rodrigo Vincenzi1, João Seda Neto1.
1Hepatology and Liver Transplantation, Hospital Sírio-Libanês, São Paulo, Brazil
Background: MSUD is a genetic disorder causing neurological impairment due to branched-chain amino acid accumulation. Liver transplantation (LT) restores metabolic homeostasis via branched-chain ketoacid dehydrogenase (BCKDH) in the partial living donor graft (PLDG). MSUD livers can be reused as domino liver grafts (DLG) since BCKDH deficiency in the DLG is supplied by enzyme production in other recipient tissues. Thee aim of the study is to evaluate the feasibility and safety of combining living donor liver transplantation (LDLT) with domino liver transplantation (DLT) as well as post-LT metabolic homeostasis for maple syrup urine disease (MSUD)
Methods: Live donors (LD), MSUD patients and DLG recipients were evaluated for compatibility through morphometric analysis for DLT, from October 2012 to November 2023, with follow-up until November 2024. Surgical outcomes as well as plasma molar ratios of leucine to isoleucine and leucine to valine were monitored in 3 periods: pre-LT, post-LT up to 90th day and 91st day up to 1 year and compared to control subjects.
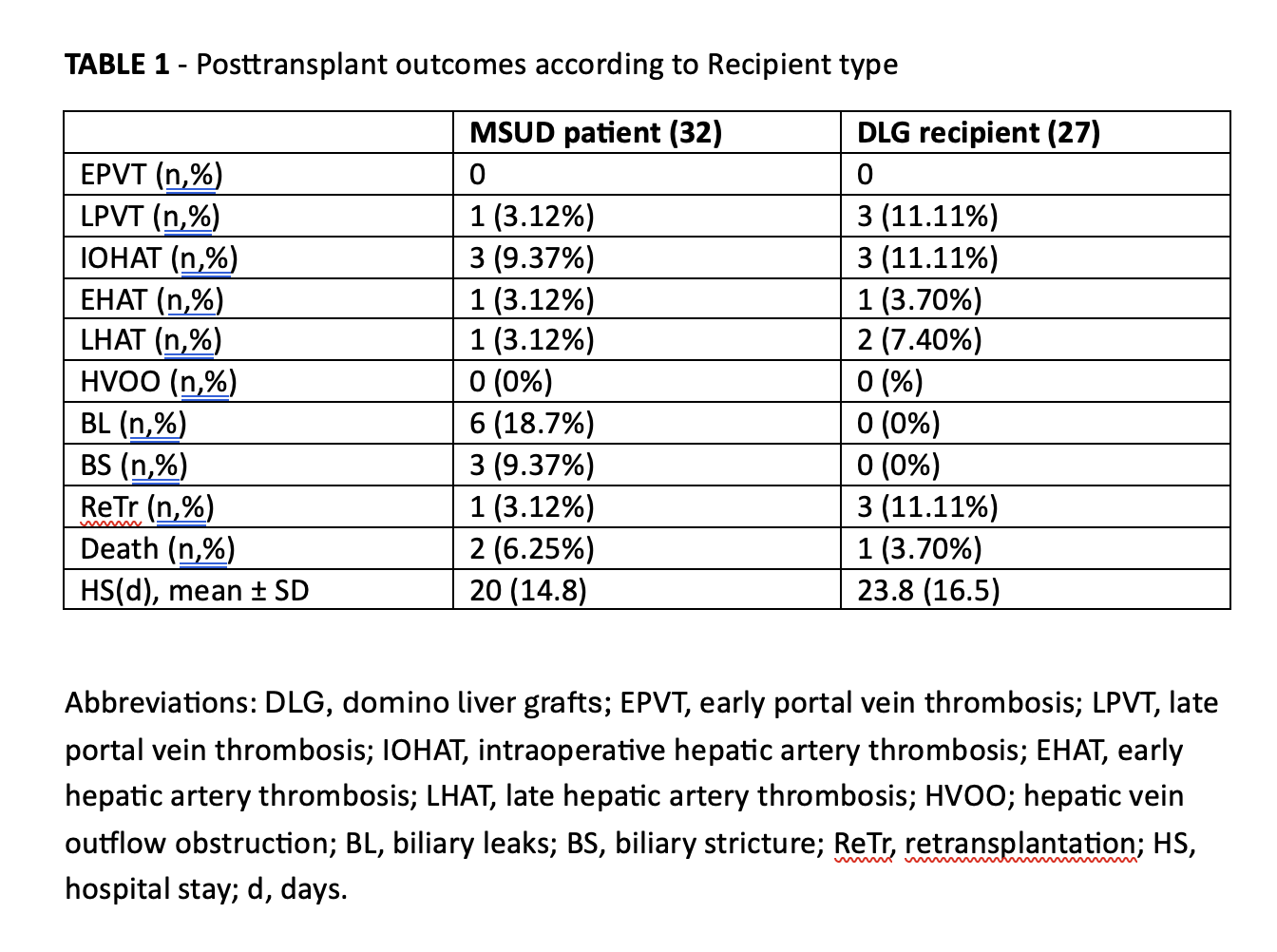
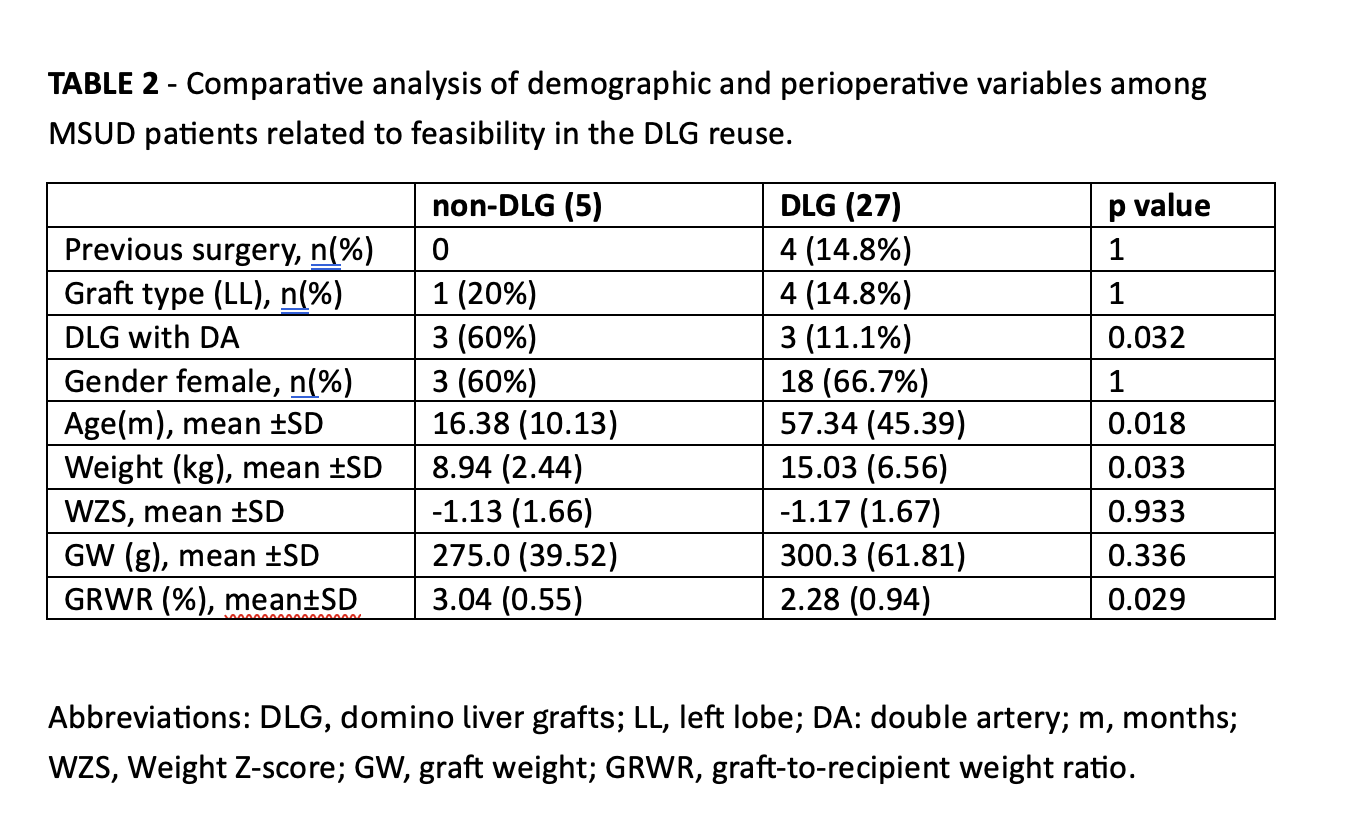
Results: Were included 32 LDLT for MSUD patients, with 27 (84.37%) grafts reused as DLT. Cumulative patient and graft survival rates for MSUD patients and DLG recipients were 93.75%, 96.3%, 90.63%, and 85.2%, respectively. Late hepatic artery thrombosis (HAT) occurred in 3.1% and 7.4% of MSUD patients and DLG recipients, respectively (Table 1). Primary factors for DLG disposal were double arteries (DA), smaller and younger MSUD patients, all related to small arterial caliber (Table 2). No increased risk related to DLG donation was demonstrated. Plasma molar ratios of leucine to isoleucine and leucine to valine demonstrated adequate metabolic control in MSUD patients after LT.
Conclusion: Combining LDLT and DLT expands the donor pool for pediatric patients while ensuring safety in MSUD treatment. Microsurgical arterial reconstruction is crucial not only in the quality of arterial anastomoses, but also for achieving a higher rate of DLG reuse. Preoperative morphometric analysis aids in planning but does not significantly impact DLG reuse decisions. The use of PLDG in MSUD patients showing metabolic homeostasis of the BCKDH activity after LT.
References:
[1] Maple syrup urine disease (MSUD)
[2] Living Donor
[3] Expanding Donor Pool
[4] Outcomes
[5] Liver transplantation
[6] Domino Liver Transplantation
Lectures by Joao Seda Neto
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Fri-19 07:00 - 07:50 |
Advances in transplant surgery | Anterior hepatic resection for infant LDLT: Medium-term outcomes | MOA 3 |
|
Fri-19 13:35 - 15:05 |
Indications for pediatric liver transplantation | Living donor plus domino liver transplantation for MSUD: expanding donor pool safely | MOA 5 |