Michael Freeman, United States
Associate Professor of Pediatrics and Humanities
Division of Pediatric Nephrology and Hypertension, Department of Pediatrics and Humanities
Penn State Children's Hospital/ Penn State College of Medicine
Is a chronic dialysis program a requirement before initiation of a pediatric kidney transplantation center: An IPTA ethics committee position statement under consideration
Tom Blydt-Hansen1, Amrita Dosanjh2, Michael Freeman3, Carl Grabitz4, Hassina Mohammed5, Marta Lidia Monteverde6, Priya Pais7.
1Pediatric, University of British Columbia, Vancouver , BC, Canada; 2Pediatric Respiratory , Rady Children's Hospital, San Diego, CA, United States; 3Pediatrics and Humanities , Penn State College of Medicine, Hersey, PA, United States; 4Department of Pediatric Kidney, Liver, Metabolic and Neurological Diseases, Hannover Medical School, Hannover, Germany; 5Anesthesia and Intensive Care , Eric Williams Medical Sciences Complex, Mt Hope , Trinidad and Tobago; 6Nephrology, Hospital JP Garrahan, Buenos Aires, Argentina; 7St John's National Academy of Health Sciences, Bengaluru, India
Introduction: End Stage Kidney Disease (ESKD) treatment requires kidney replacement therapy (KRT), either with dialysis or a kidney transplant. Kidney transplant restores function and improves quality of life (QOL), whereas chronic dialysis is similarly lifesaving but more costly and associated with lower QOL. Chronic dialysis is often regarded as a bridge to a transplant. For programs initiating KRT programs, however, resources limitation may not be conducive to implementing both transplant and chronic dialysis services. This draft position statement is intended to advance discussion on whether it is justifiable to initiate transplant services, when chronic dialysis services are not available.
Methods: The IPTA Ethics Committee formed a working group, involving members of the IPTA Ethics, Outreach and Publication Committees. The working group performed a literature review and held several one-hour virtual meetings via Zoom for discussions and analysis. An initial position statement draft will be reviewed by the committee and submitted for commentary by the IPTA membership, which is the purpose of this abstract.
Key considerations: The main arguments for starting first with a transplant program are reduced ESKD-related comorbidity, improved survival, QOL and lesser cost compared with dialysis. Transplant costs are higher in the first year and decline thereafter. There is less care burden for families (physical, emotional, and financial). However, donor scarcity means some children may not survive to until a donor is available and may have advanced uremic complications at the time of transplant. Perceived requirement for chronic dialysis is based on its availability as a vital bridge to transplantation, and chronic rescue KRT if a transplant is unsuccessful. It most effectively assures that all children with ESKD may have access to a lifesaving KRT modality, regardless of transplant eligibility or access to a donor. Dialysis programs are more costly, but the technology and supplies are more readily available, even in less developed healthcare systems. Both dialysis and transplantation require advanced training, expertise and infrastructure for support, and access to partnering adult transplant or dialysis programs is viewed as a critical facilitating factor. Resource constraints, health system priorities and societal beliefs (e.g. about organ donation) will vary importantly across jurisdictions and will differently impact on local feasibility of each modality.
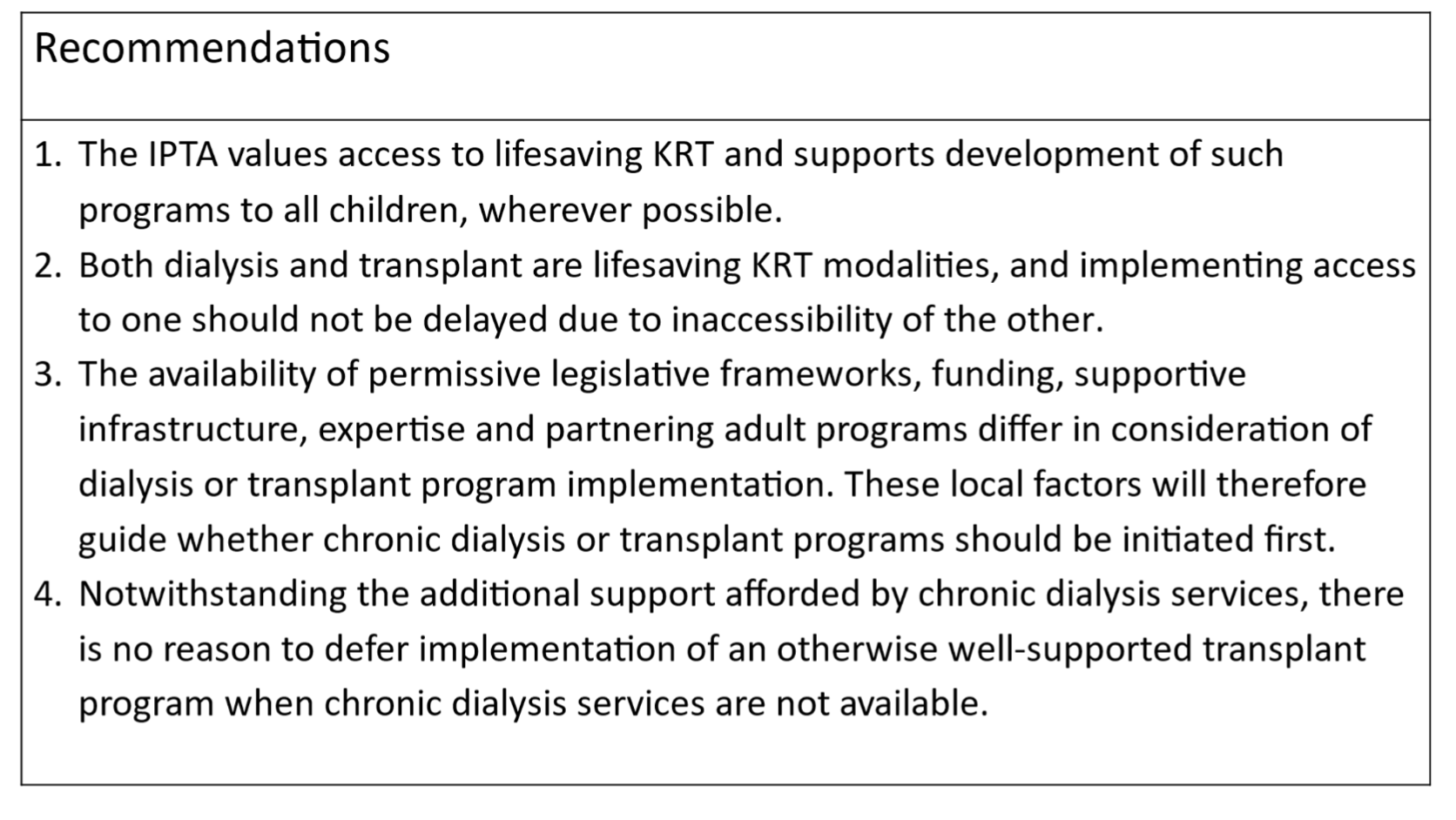
Conclusion/Recommendations: The working group will be seeking feedback and commentary from the IPTA membership and society leadership. Formal recommendations are being developed, and may include the following:
References:
[1] Chronic dialysis
[2] Kidney transplant
[3] Ethics
[4] ESKD
Lectures by Michael Freeman
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Thu-18 16:00 - 17:00 |
Best Ethics and Allocation Abstracts | Is a chronic dialysis program a requirement before initiation of a Pediatric Kidney Transplantation Center: An IPTA Ethics Committee position statement under consideration | MOA 3 |